
Searching this forum for this subject proved a little difficult but thanks to methodman and rick_b’s posts I got some traction on some previous discussions (but they’re not exactly on point so I won’t bother you with the links). In particular ricky_b has an earlier post that references a NYTimes article about the ‘dual risk’ for TS from which includes hormone injections. Unfortunately the article referred to is ten years old and I am looking for more current information. If for no other reason, reusing needles just sounds painful to me – every time a needle’s tip is touched it gets a little duller. In particular, hasn’t more and better information on these risks changed the way TS approach both escorting and their transformation from one sex to another?
Hopefully methodman is right and we are all informed adults but the knowledge base is forever changing and behaviors should be modified accordingly. I don’t agree with ricky_b that the hobby is necessarily ruined – each hobbyist chooses a level of risk to suit their individual comfort level, hopefully that choice is well informed and based on accurate information. One of ricky_b’s posts is in a thread discussing the rising price of TS services – do higher prices mean that TS can afford and are practicing safer hormone therapies? Let’s certainly hope so, but I’d still like to hear more about it. Kylie (post-op) and Mandy had some interesting things to say but none were specifically on this point about IDU risk:
http://www.theeroticreview.com/discussion_boards/viewmsg.asp?MessageID=18365&boardID=19&page=
BTW it was one of ricky_b’s earlier posts that lead me to the TS provider who is also HIV+ and continues to offer escort services – you can search for it yourself.
TS Alter Ego very succinctly supported my observed general rule that hobbyists try to be selective in seeking out escorts that are known to practice safe sex and avoid apparent drug users. This gets discussed quite a bit in reviews and in this forum – reviewers almost always report on safe sex practices and ‘weird’ behaviors. However, since TS are most likely using injected hormones, this is a risk that I still don’t think is being discussed openly enough.
Take care,
TS Tempted
-- Modified on 12/22/2006 9:39:24 AM
As everyone knows I am a relative ‘newbie’ to this forum. Accordingly I have been very appreciative of everyone’s patience and indulgence with my ‘newbie’ posting activity. Recently I posted some news about male circumcision (see related link below) which has motivated me to think a little deeper about the subject of STD’s in the context of the TS community. We flirted with the subject a little bit at that time but I would like to solicit additional comment and information from the forum on a particular subject related to TS.
Specifically the ‘elephant in the room’ that I am curious about is TS and injected drug use or IDU. My concern is not just with the stereotypical IDU, such as recreational drugs, but is more broadly based, e.g. a diabetic who must inject themselves with insulin on a routine basis would be an ‘IDU’ in this context. Nobody seems to want to talk about this anywhere, much less here (and yes I have tried some searches of this forum on this subject).
Perceived IDU Risk in the TS Community
My understanding is that most people in the process of transitioning from one sex to another use a variety of reasonably intensive hormone therapies for a period of years during this transition. Further it is my understanding that most of these therapies involve INJECTED hormones.
Notwithstanding the issue of expense, if a TS is pursuing a hormone therapy treatment regime under the direction of a physician through prescription, no worries, they probably have access to new sterile syringes for each administration of hormones. However there appear to be many who may engage in these treatments on a ‘do-it-yourself’ or DIY basis (I realize now that I was being naïve but I was nevertheless surprised to find entire websites out there dedicated specifically to DIY hormone therapies for TS). My concern is that this opens the door for unsafe IDU from reuse or sharing of needles and other hormone supplies and paraphernalia much as it might for the stereotypical recreational drug user.
In addition, it is also obvious that most TS also engage in some form of body modification to alter their appearance closer towards their preferred sex. Again this opens a door for unsafe practices if such a person pursues such enhancement in the form of DIY or from illicit providers of these services. For example, one form of questionable body modification that I have read about is silicone injections, but again I haven’t found a whole lot of information readily available on this topic.
Risk Mitigation in ‘The Hobby’
If there is such a thing as consensus in the ‘hobbying’ community it would appear that providers and hobbyists with a reputation for EITHER unprotected penetrative sex OR IDU are generally to be avoided. There seems to be varying opinions about unprotected oral sex – most seem comfortable with the risk of BBBJ and DATY, but CIM and NQNS are ‘off the menu’ for many. Providers and hobbyists with a reputation for such behaviors may even be specifically avoided by some. Indeed, when screening new clients GG providers have been known to turn down new clients if they see TS reviews under their handles on the boards – there have been some previous discussions of that subject in this forum, prompting the use by some of alternate handles for posting TS versus GG reviews.
Many years ago when I fist became interested in ‘the hobby’ and realized that so much information was available on the internet one of my first lines of research was into STD’s, and obviously particularly, HIV. Interestingly, one conclusion that may not be wholly unreasonable after reviewing a lot of this information is that, if someone (either provider or hobbyist) is following the proscriptions outlined above, the risk of contracting HIV, may be no greater that that of the general public. Now remember the ‘general public’, by definition, will include high risk behaviors such as IDU, unprotected penetrative sex and outright accidental exposures. The point being that while participation in the hobby is obviously increasing risk by increasing contact with a multitude of partners, this risk appears to be mitigated significantly through safe sex practices (and avoidance of contact with those who have may a reputation for high risk behaviors such as unprotected sex and/or IDU?).
Invitation for Discussion and Additional Information
So now we return to the TS question. I’ve been looking into the subject of HIV and TS for sometime now and still have more questions than answers. Unfortunately there appears to be almost a total dearth of specific information about TS and the incidence of STD infections in this community. Since being a TS usually means some form of hormone therapy and body modification, does this implies a higher degree of IDU risk in this community?
This perceived IDU risk is in addition to the obvious one of penetrative anal sex. We do seem to spend a lot of time discussing the later but don’t seem to want to discuss or attempt to discriminate safe behaviors from unsafe ones with respect to the potential IDU risk. I would like to ask the participants in this forum to help me out with specific comments to correct my understandings above and/or provide references to additional information on these subjects (which I am finding fairly difficult to find).
Maybe there is no elephant and it is all just my imagination…
Regards,
TS Tempted

A lot of this has already been discussed in the related link below. That post had links to summaries of the latest CDC statistics – worth checking out if you’re interested. HOF correctly pointed out in his reply to that thread that over 51% of new HIV/AIDS cases have male-to-male sexual contact as some contributor to contraction of the disease (unprotected anal sex seems implicit in this statistic).
In fact over 70% of the new cases each year are from a combination of either male-to-male and/or IDU. As HOF pointed out very vociferously statistics has many flaws and biases. My guess is that much of the 30% that’s left might even track back to this 70% if it was possible to do that somehow.
If you dig further into the CDC information you quickly realize that in addition to the male-to-male and IDU factors there are other statistically significant contributing factors - race, age, other STD status and sex. In summary, depending on how you look at the #’s, most of us in the U.S. are several times more likely to be murdered than to contract HIV (the FBI has the murder statistics somewhere on their website but I forgot to record the link).
Hypothetical or Subjective Risk Scale
In his reply to the post in the related link below, goethe was quick to point out that risk for IDU’s could be significantly reduced by the use of new sterile needles – I would add that it should also involve no sharing of other IDU supplies and paraphernalia that could contaminate the drugs or syringes being used. Okay, so this sparks another line of thinking. Just what are the various risk factors and how do they compare?
I am not aware of anywhere that such a ranking of risk on any type of scale has been done and would be very interested if anyone could provide additional information along these lines with scientific or biological support. Not being shy about these things I have put together a scale that is purely subjective, with no basis other than my own personal and anecdotal review of the subject. I would appreciate your comments and any corroborating or contradicting information. My ranking, where 1.00 is a blood transfusion (and assuming, in the case of sexual contact, no obvious open sores, lacerations, etc.) is as follows:
1.00 Blood transfusion (mitigated thru testing and screening to 0.10)
0.98 IDU and surgical (mitigated thru sterilization and use only once 0.10)
0.95 Unprotected anal sex - receiving
0.75 Unprotected vaginal sex – receiving
0.55 Unprotected anal sex – giving
0.50 Unprotected vaginal sex - giving
0.45 NQNS - giving
0.35 CIM – giving
0.25 BBBJ/DATY – giving
0.22 Oral sex - receiving
0.20 General level of risk population as a whole
0.15 Protected sex all types (latex, non-oil lubricants, no cheating, no breaking)
0.05 Abstention (sh*& happens category – as long as you are alive on this planet the risk can never be zero)
Your thoughts on the scale, and the assumptions and conclusions that went into it would be most appreciated.
Other Observations
I don’t even know where to put rimming. Maybe between BBBJ/DATY and CIM – any better/other suggestions? Certainly rimming should be up there for other things such as hepatitis?
Yes, one strange conclusion from my ranking is that, contrary to popular myths about prostitution, practicing safe sex in ‘the hobby’ could indeed be safer that the general level of risk in the overall population.
My own observation is that many providers and hobbyists are comfortable in the 0.30 range, i.e. BBBJ/DATY is “on the menu”. They would also probably avoid known bare-backers and IDU and maybe even NQNS.
Providers do continue to provide after becoming aware that they are HIV+. There are some court cases to this effect available from a Google search and if you search this forum you can find a recent example of a TS provider that publicly admits to being HIV+ in another venue but apparently maintains an escorting practice with an ad on Eros that has no mention of her HIV status.
Everyone gets tired of condoms eventually. I am not so naïve as to think that there aren’t “exclusive” arrangements out there with respect to unprotected sex or even a price (which may include non-pecuniary consideration such as testing) at which some will participate in such high risk behavior. If you find someone you can ‘trust’ with an ‘exclusive’ or ‘high risk’ relationship all this may really mean is that they share a preference for the same risk profile outside the relationship as you do. If you can at least assume that they will stringently practice safe sex on the same terms as you then I guess your exposure with them is no greater than your own, other than the ‘implicit exposure’ to their partners in addition to your own.
The Elephant in the Room
It is my impression that most hormone treatment is IDU but also various forms of body modification and beautification such as silicon injections, etc., may also be IDU. Apparently DIY practices outside ‘normal’ medical and health industry practices is not uncommon. If so, what is the risk for TS? Nobody seems to be talking much about this anywhere, much less here.
Where does IDU for DIY hormone therapy and body modification fit on this risk scale and what are its mitigants? How does it vary in different regions outside North America, such as Europe and Latin America? Hormones and body modifications are ‘personal’ and not ‘party’ events so sharing of needles and supplies are not so obvious to me, but I have no idea how these may be obtained, what their sources may be and how we should look at these with respect to adherence of proper sterilization practices.
Comments on the risk scale, my perception of IDU-type risk in the TS community and links to additional sources of information would be welcome.
Take care out there,
TS Tempted
After reading through both posts, it makes sense to me that I feel most comfortable with TS women who are under a doctor's care (no DIY treatment) and who show absolutely no signs (emotional or physical) of drug use. But that's easy for me to say. My TS attraction has evolved to the point where it seems very specific, so that after some slightly reckless experimentation with TS girls which ended a few months ago, I am now able to just say no when I feel the slightest bit uncomfortable. But I realize that aint the way of the world for many of my fellow hobbyists. A late night out, a few stiff drinks, and all of a sudden that ad in the Village Voice doesnt look so bad. The next thing you know you're walking up three flights of stairs in a tenement to meet a cirsus sideshow refugee who immediately begins upselling you for the privilege of sucking her uncovered half-stiff personhood.
It's a tough hobby, guys, but there are some real sweethearts out there. TST's painstaking analyses of the best of the best hold many valuable clues. Be courageous; be selective.
TSAG
I'm sure you mean well my friend... but... the reason no one wants to talk about it is because its a lot of mental masturbation.
We are all presumably adults presumably aware of the risks in the thing we do.
Again presumably we mitigate them to our own individual satisfaction and I again presume are not interested in examining the topic in such painfully minute and pedantic detail as you seem to be interested in.
Hope that helps.
no help at all, try feeding your ego at McDonalds. Ok, so you have a firm grip on what's clear to most. There is risk involved. All this guy above is doing is trying to point out the level of risk. I'll take it ahead another step and say that the risk is beyond reason and the hobby is ruined. Even several of the more successful escorts admit that they are scared shitless about aids.
Oh the sky is falling and we're all scared and unaware.
Thanks, Ghandi any more tips.
about how many std's you end up getting, have fun!
Searching this forum for this subject proved a little difficult but thanks to methodman and rick_b’s posts I got some traction on some previous discussions (but they’re not exactly on point so I won’t bother you with the links). In particular ricky_b has an earlier post that references a NYTimes article about the ‘dual risk’ for TS from which includes hormone injections. Unfortunately the article referred to is ten years old and I am looking for more current information. If for no other reason, reusing needles just sounds painful to me – every time a needle’s tip is touched it gets a little duller. In particular, hasn’t more and better information on these risks changed the way TS approach both escorting and their transformation from one sex to another?
Hopefully methodman is right and we are all informed adults but the knowledge base is forever changing and behaviors should be modified accordingly. I don’t agree with ricky_b that the hobby is necessarily ruined – each hobbyist chooses a level of risk to suit their individual comfort level, hopefully that choice is well informed and based on accurate information. One of ricky_b’s posts is in a thread discussing the rising price of TS services – do higher prices mean that TS can afford and are practicing safer hormone therapies? Let’s certainly hope so, but I’d still like to hear more about it. Kylie (post-op) and Mandy had some interesting things to say but none were specifically on this point about IDU risk:
http://www.theeroticreview.com/discussion_boards/viewmsg.asp?MessageID=18365&boardID=19&page=
BTW it was one of ricky_b’s earlier posts that lead me to the TS provider who is also HIV+ and continues to offer escort services – you can search for it yourself.
TS Alter Ego very succinctly supported my observed general rule that hobbyists try to be selective in seeking out escorts that are known to practice safe sex and avoid apparent drug users. This gets discussed quite a bit in reviews and in this forum – reviewers almost always report on safe sex practices and ‘weird’ behaviors. However, since TS are most likely using injected hormones, this is a risk that I still don’t think is being discussed openly enough.
Take care,
TS Tempted
-- Modified on 12/22/2006 9:39:24 AM
I realize that I am still at risk for boring everyone but below is an interesting (to me anyway) chart that shows the incidence of newly reported HIV/AIDS cases by year from 1981. Please remember I am not an expert but a few things seem obvious to me:
1. Total new cases may be rising from 1981 to early ‘90’s primarily because of a reporting phenomenon - medical practitioners are becoming more aware of the disease, reporting the correct diagnosis on more timely basis and the health industry is developing and improving tests for HIV
2. Since the peak, total new cases annually have fallen dramatically, particularly in the highest risk areas of male-to-male sexual contact and IDU
3. The total number of new cases has generally leveled off but is also slightly trending upwards since the millennium
4. Unfortunately, heterosexual cases never experienced such pronounced declines and while they have generally leveled off since the mid-90’s they are never-the-less still trending upwards
Whatever the specific underlying reasons, we are fortunate in the U.S. to have enjoyed the overall dramatic decline in new cases since the early ‘90’s. Obviously education and awareness has had its impact on high risk behaviors. One reason the newly reported infection rate may be proving resistant to further decline is immigration – we simply may be importing the disease from other areas of the world where it is more prevalent.
I still think we can do even better in this country and lead the way for the rest of the world to get a handle on this tragic problem. This requires us to be vigilant and continue to openly discuss the issue and the risk factors. In particular, I think ‘the hobby’ has a leadership role in this process. It goes with out saying the number of different reasons that people seek out escorts are as numerous as there are people doing it but there is also something going in the process that should not be overlooked. If you want to learn how to play tennis, particularly if you want to learn to play better, what do you do? You call the local professional and schedule an appointment for a lesson. Believe it or not, ‘the hobby’ is educating and informing people not only about how to have ‘better’ sex but how to do it more safely.
Okay maybe tennis isn’t the best analogy because it isn’t normally a life-threatening activity so how about sky-diving? Thousands of jumps are being made each day and accidents are rare. Why? Because everyone jumping out of airplanes has taken lessons from professionals. Alright, so you can’t jump out of an airplane without a license, so maybe it isn’t the best analogy either - since the equipment comes standard just about anyone can have sex. As goethe pointed out before, just because an activity is ‘high risk’ doesn’t mean that risk can’t be reduced, mitigated or maybe even eliminated.
Again, I would submit that ‘the hobby’ has a leadership responsibility and can have a significant impact (though maybe an unacknowledged one) throughout our society by openly discussing and promoting risk mitigating behaviors. Not just with respect to safe sex but including those with respect to IDU generally and IDU specifically in the context of hormone therapies for TS.
Regards,
TS Tempted
-- Modified on 12/22/2006 9:36:51 AM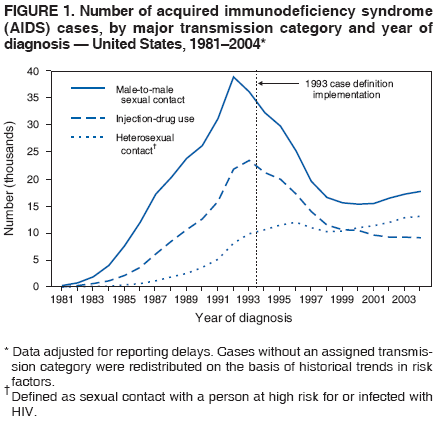
injection is entirely different. When you inject a sterol based hormone like progesterone or estrogen you do not inject it directly in the bloodstream through a vessel. The hormone is esterified so it can be dissolved in fatty oil and is injected into a muscle. With an intramuscular injection, you do not want to hit a vessel. The protocol is to pull back on the syringe plunger and look for air bubbles or blood. If you see blood when pulling the syringe plunger back you need to pull the needle and syringe out and inject elsewhere. There is no blood in the syringe or needle at any point in a proper intramuscular injection.
With an intravenous injection, you want to see blood in the syringe when you pull back the plunger as that means you entered the desired vessel.
Blood being one of the media that hosts HIV kept in a vaccuum in the syringe after an IV injection(IntraVernous) is different than reusing an IM injection(IntraMuscular) as no host media is kept in a vaccuum.
-- Modified on 12/28/2006 6:54:19 AM
HOF, how often do you get blood in the syringe from IM injections? If so, and there is reuse of the syringes, don’t we have the same risk?
You also talked about host media kept in vacuum which I would like to understand better. Is HIV so fragile outside of the body that unless maintained in a vacuum it will degrade rapidly? If so, why is there such a concern in the literature with other IDU paraphernalia as well as the syringes?
Thanks,
TS Tempted
HIV is a virus that does not contain all the biological organs necessary to insure it's survival in a hostile enviornment. Some even argue whether or not viri are truly living organism as essentially all viri are just transporters of genetic material encapsulated in protein, hence the frailty.
I'm sure you can theoretically get blood in the syringe after an IM injection and in practice it happens, but it is often exposed to air. The other problem with reusing IM needles compared to IV needles is the fact that IM needles are generally thinner (probably 23 or 22 gauge) for most IM injections. An IM needle has to pass through much more tissue than in IV. They become very dull and bent after an injection. If you reuse you are looking at progressively more painful injections and due to distorions in the barrel of the needle it may become impossible to inject.
The concern with IV injection is that you intentionally draw blood into the syringe to ensure a vein was injected and the syringe maintains a vaccuum and an HIV friendly enviornment.
Maybe it’s an Ass instead and the ass is me (LOL)? Or maybe it’s just that needles really get my attention. Thanks for your info HOF. What you say makes very good intuitive sense (of course). A lot of this is particularly hard to figure out for those of us not trained in the health sciences. We are very lucky indeed that as lethal and tragic as HIV is, it is also somewhat fragile.
It has always been my observation that on most topics there is too much discussion about ‘what’ and not enough ‘why’. I find that if I can get a good understanding of ‘why’ then the ‘what’ seems pretty obvious, but unfortunately for me the world seems to work with a focus on the ‘what’ instead. Why is that (uh oh here I go again…)? Is it that the smart people think the rest of us are too stupid to understand and that it is better to just give us an answer instead of the tools that come with understanding? “If you give a man a fish he will eat for a day. Teach a man to fish and he will eat for a lifetime.”
Okay, so where do I conclude that this fits on my risk scale? I have been reading more about oral sex risks and I would revise my scale for NQNS/CIM downwards a little and BBBJ/DATY upwards a little to maybe around 0.30 +/- 0.05. So maybe TS DIY hormone and body modification falls somewhere slightly above this risk level as there do seem to be some issues but nothing more significant that good hygienic practices wouldn’t address?
Regards,
TS Tempted
Re-used ear piercing guns as seen in most shopping mall jewelry pagodas and stores.
Ewww, I just knew there was a reason I didn’t like those places. While I can appreciate a tasteful piercing, nice piece of jewelry and even a finely crafted tattoo, my aversion to these places probably has as much to do with my general emotional problem with needles as my intellectual appreciation for the risk of infection…